
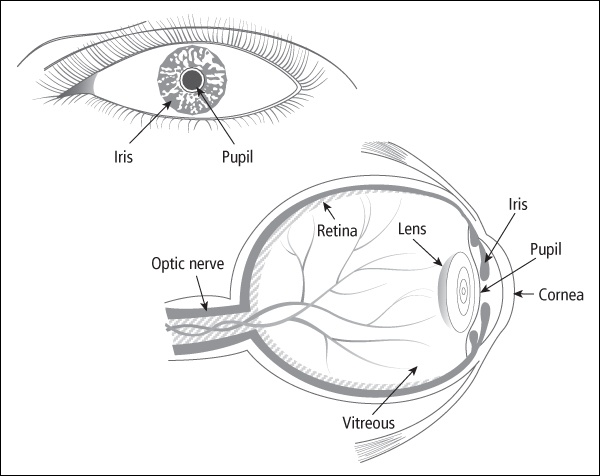
The eye is the organ of sight. This nearly spherical body has numerous layers. At the front is the transparent cornea; through the cornea the colored iris is visible. The space between the cornea and the iris is the anterior chamber, which is filled with a clear fluid called aqueous humor. In the center of the iris is a space called the pupil that contracts or expands to control the amount of light entering the eye. Directly behind the pupil is the lens of the eye. The cavity behind the lens is filled with a gel-like substance called the vitreous humor. The thin layer that lines this cavity is the retina, which detects the light signals that enter the eye. The optic nerve transmits light information from the retina to the brain. Figure 10-1 shows the anatomy of the eye.
Organ damage
The eye can be damaged by radiation, treatment with steroids, or surgery. Vision can also be harmed if the optic nerve is damaged anywhere between the eye and the brain, which can happen from radiation, a tumor pressing on the optic nerve, or a tumor in the brain causing high fluid pressure around the brain and optic nerves. In addition, tumors in the brainstem (where the brain meets the spinal cord) can cause problems with eye movement or double vision.
When a cancer is in the eye, as in retinoblastoma, the affected eye might have to be surgically removed (called enucleation); this occurs less often now than in the past because of newer radiation techniques and chemotherapy protocols. Small and medium-sized retinoblastomas are often treated with some combination of chemotherapy, cryotherapy (freezing treatment), and photocoagulation (laser treatment). Large or advanced tumors may require enucleation.
Thirty years ago I was diagnosed with retinoblastoma when I was 18 months old. They thought it was the non-hereditary form because it was one tumor in just one eye. The eye was surgically removed, and I had no chemotherapy or radiation. I have no late effects other than wearing a prosthesis and having vision in only one eye.
The eye is exposed to low-dose radiation during total body irradiation (TBI) prior to some types of stem cell transplants. High-dose radiation is used to treat retinoblastoma, rhabdomyosarcoma, and other tumors around the eye. The eye may also be exposed to radiation given to treat brain tumors or leukemia.
Some common problems of the eye after treatment for childhood cancer are as follows:
-
Hypoplasia (slowed growth of the bones around the eye)
-
Cataracts
-
Dry eye
-
Shrinkage of the lacrimal duct, which drains tears from the eye
-
Loss of vision
Ten years ago my newborn daughter was diagnosed with retinoblastoma in both eyes. She had one eye removed and both eyes radiated with 2200 cGy (centigray). Two years later the tumors returned in her remaining eye. The tumors regrew only 3 weeks after chemotherapy ended, so she had more chemotherapy. When that course had to be cut short due to side effects, they decided to remove the remaining eye. She has some learning problems from the radiation and wears two prosthetic eyes.
A common late effect is slowed growth of the orbits (eye sockets), which are the bony structures in the skull that protect the eyes. Each orbit is made up of seven bones, all of which can be damaged by radiation. This late effect is most noticeable in survivors who were treated at a very young age with more than 4000 cGy in the areas of the growing bones. Survivors with severe hypoplasia sometimes benefit from reconstructive surgery after the bones in the face are fully grown.
Joseph had 12 cycles of chemotherapy and 5000 cGy of hyperfractionated orbital radiation (twice daily for 6 weeks). With this treatment regimen, almost all of his above-the-neck side effects will be due to the radiation, not the chemotherapy drugs. Many of the side effects of radiation on the body are, of course, delayed for months or even years. He will suffer “bony hypoplasia,” which means that the bony structures that absorbed radiation (in this case, his right temple and in and around the right orbit) will not grow any more, so his face will look increasingly asymmetrical as he grows up. The doctors are optimistic that it won’t be too noticeable since he was turning 5 when treatments were done.
Cataracts—when the lens of the eye becomes opaque—are a frequent late effect of radiation treatment. Cataracts can cause vision loss, but they can often be treated with surgery. Higher doses of radiation cause more damage and shorten the time before cataracts appear. Cataracts appear earlier and become more severe if the child was treated at a young age. In addition, single, larger doses of radiation cause cataract formation more often than the same total dose given in several smaller fractions. Long-term steroid use (including prednisone and dexamethasone) or busulfan chemotherapy can also cause cataracts.
Naomi has had cataracts for the past 6 years as a result of high-dose prednisone and TBI from her BMT (bone marrow transplant). The cataracts are quite different from what we think of in terms of the elderly—they are not visible on the outside of the lens and in fact don’t impair her vision. She has maintained 20/20 vision in spite of the cataracts, and there is no indication that that will change. The one thing that she does find is that the contrast of light to dark is affected. She can easily read the ophthalmologist’s chart when it has black letters on a white background. The same chart done in tones of gray is very difficult for her to read. Also, white chalk writing on the blackboard is more difficult to read at times. Light really bothers her, either the bright summer sun or the reflection of the sun off the snow. The light hits the cataracts and disperses the light in the eye. So Naomi really needs to wear very good quality sunglasses with good UV (ultraviolet light) protection when out in bright sunlight.
Graft-versus-host disease and/or radiation can cause mild to severely dry eyes. Symptoms include irritation, burning, pain, blurred vision, sensitivity to light, and the feeling that a foreign body is in the eye. Dry eyes can be eased by using artificial tears.
Like most children who are a couple of years out of treatment, Joseph’s scans and doctor visits are now more related to dealing with the long-term effects of the rhabdomyosarcoma cure than the disease itself. He has a big cataract on his right eye from the radiation, and his vision in both eyes is rapidly getting worse. He still needs eye drops every 2 hours all day because of damage from the radiation, and he has terrible problems with light sensitivity. But he always manages to compensate and doesn’t let anything get in the way of his reading or play or computer games.
Loss of vision can involve central vision (the detailed vision used for reading), or the peripheral visual fields (side vision). Loss of peripheral vision can result from damage to the retina or optic nerve, or damage to the visual areas of the brain from brain surgery.
I had an ependymoma (brain tumor) 6 years ago when I was 8 years old. I have visual field cuts. I don’t see the whole picture that other people see. My peripheral vision is limited, as well as my lower field. This causes me a lot of problems. For example, I can’t walk to school by myself right now because I don’t notice cars moving on my left side as well as other unpredictable occurrences in city streets. I have to try to remind myself to keep turning my head. I can’t follow any visual cues such as pointing, but instead rely on verbal instructions. I’m starting high school this year, so I’ve been going to the school with my mobility instructor to walk around and memorize the layout. The vision I do have is good, but it’s only a fraction of what other people see.
Less common late effects to the eye or eye socket from radiation can include:
-
Permanent loss of the eyelashes.
-
Hemorrhaging of small damaged blood vessels in the retina (telangiectasias), typically occurring 3 to 5 years after treatment with more than 3000 cGy.
-
Adhesions and scarring that limit the ability of the lids to fully close, making the eyes drier.
-
Inflammation of the cornea (called keratitis), with sensitivity to light and pain at the surface of the eye.
-
Ulcers, holes, or scarring of the cornea after treatment with more than 4000 cGy.
-
Glaucoma (increased pressure within the eye), which can also be caused by steroid use.
-
Secondary cancers.
Any of the late effects described in this section should be treated by an ophthalmologist skilled in treating survivors of childhood cancer.
At the time he received the 5000 cGy to his eye, we were told Joseph would probably lose some vision in the treated eye, but they said the effect might be anywhere in the range from barely noticeable to completely blind. It’s been 2 years and so far Joseph’s vision tests at 20/20. But when I asked the ophthalmologist at the last visit if that meant we were out of the woods, he grimaced and shook his head. He’s still expecting something to show up and says we’re not far out enough yet to know what the extent will be. Darn it.
Surgery, stroke, and some medications can also cause problems with the eyes and vision. If there is damage to the part of the brain that controls the muscles that move the eyes, this can result in an eye that does not move normally, and the two eyes not being lined up with one another. If this happens at an early age, the brain may start to ignore one eye, and the eye can lose vision as a result (called amblyopia). Amblyopia may need to be treated with patching therapy (patching the good eye to improve vision in the eye that is not being used). Surgery may help improve the alignment of the eyes, but it can’t always restore a full range of movement.
Our son had an epidural hematoma (bleeding into the brain) after his surgery to remove a medulloblastoma. One side effect from this was that the left side of his face is partially paralyzed, and his left eye turns in toward his nose. One ophthalmologist told us that surgery can put it back in the right position, but it would forever remain fixed in that one place. After a year of therapy, he can now move the eye up and down and to the right. He can move it a bit toward the left, and his vision has improved.
• • • • •
One of our daughter’s seizure medicines caused vision disturbances. She developed tunnel vision and had trouble seeing. We changed the drug and it went away. She’s at risk for cataracts from her cranial radiation, so we go to the eye doctor every year.
Signs and symptoms
When children are old enough to talk, and certainly by school age, visual disturbances are usually detected and treated. However, if changes are gradual, a child may get used to them, and identification of visual late effects can be delayed. The following are signs and symptoms of late effects to the eye: 1
-
Blurry vision
-
Double vision
-
Blind spots or a decrease in visual field (range of vision)
-
Increased sensitivity to light
-
Difficulty with night vision
-
Floaters across the field of vision that change or light up
-
Pain in the eye
-
Persistent dry, scratchy eyes or eyelids
Screening and detection
You should be seen regularly by an ophthalmologist with experience treating survivors of childhood cancer if you:
-
Had total body radiation.
-
Received high-dose radiation to one or both of the eyes or nearby structures.
-
Received radiation for a brain tumor or leukemia that included an eye in the radiation field.
-
Used steroids for a prolonged period.
The ophthalmologist should perform a thorough evaluation that includes evaluation of vision, a test for glaucoma, checking for cataracts, and examination of the retina.
My 10-year-old daughter is 6 years out from her retinoblastoma relapse. We see the oncologist and ophthalmologist every 6 months for a checkup. Because she has a 30 percent chance of developing a secondary tumor, she has careful examinations and occasional CT (computed tomography) scans. When she started having headaches, she had an MRI (magnetic resonance imaging). Our doctor is great. When something worries us, she checks it out thoroughly. My daughter has a prosthesis for her eye and needs to go back every 6 months to get it resized and built up.
Survivors not at high risk for eye damage will usually have a brief eye examination as part of their yearly follow-up examination. This should include a visual examination of the eyes and a vision test using a Snellen letter chart, or a picture chart for children who cannot read letters. Even children as young as age 3 can identify simple pictures on charts specially designed for preschoolers. Any abnormalities should result in a referral to an ophthalmologist.
Joseph has not had cataract surgery, but it is expected that he will develop one or more cataracts in the next year or so because of the 5000 cGy directed at the rhabdomyosarcoma in his orbit. We see a pediatric ophthalmologist frequently to stay on top of the late effects, and so far so good. Right after diagnosis the doctors explained the probability of cataracts and the surgery that is done to remove them if they are in the line of vision.
For additional information about vision tests that you should have based on your specific treatment, you and your healthcare provider can refer to the Children’s Oncology Group’s survivorship guidelines at www.survivorshipguidelines.org .
Medical management
If you have any visual changes, you should be followed by an ophthalmologist skilled in treating survivors of childhood cancer. If you have cataracts or glaucoma, you may need glasses, medications, and/or surgery. Survivors who had one or both eyes removed will need a series of well-fitted prostheses as they grow, and education about caring for the prostheses.
A survivor’s healthcare team should also provide referrals to resources to assist with adjustments related to limited vision. Special arrangements should be made with schools to provide preferential seating, eyewear protection, and other necessary accommodations. Long-term follow-up clinics can provide detailed information about educational regulations and opportunities for young people with visual impairments. For more information about education, see Chapter 4 .
My daughter has cataracts in both eyes due to the total body radiation from bone marrow transplant. Katherine is given dilating drops every morning so she can “see” around the cataracts. Because the dilating drops paralyze the focusing mechanism, Katherine wears bifocals. One lens is for normal vision and the other for reading.
• • • • •
My daughter was having a lot of problems in kindergarten seeing the board and doing her work. Even though we had been to the ophthalmologist 4 months before, we went back. Her eyesight had deteriorated considerably and was now 20/400 in the one eye, while the other was still 20/30. When we discussed the surgery, the doctor told us that if the capsule had been damaged by the radiation, a replacement lens could not be inserted, and he would not know until they got in and looked. Luckily, the capsule was fine and the new lens works great. Her eye now is 20/80.
Artificial tears and ointments are used to protect the cornea and preserve vision in survivors with chronic dry eyes. A severe problem with dry eyes can sometimes be fixed by closing the tear draining ducts with either plugs or surgery (called punctal ligation). It also helps to avoid anything that contributes to dry eyes such as wind, fans, smoke, low humidity, or air conditioning.
After our son’s surgery for medulloblastoma, the left side of his face was partially paralyzed. His left eye remains partially open all the time. When he first came home, we put drops in his eye every 3 hours and eye lubricant at night. Now we just watch it and use drops if his eye gets red. When the house is dry in the winter, we need to use more.
Survivors who develop corneal ulcerations as complications of dry eyes may need to be treated with antibiotic eye drops.
The major side effect we were warned of that has been a constant problem since treatment has been the radiation damage to the lacrimal gland in his right eye. He needs constant lubrication in that eye because it provides very little moisture by itself. It took us a long time to come up with the best way to keep his eye consistently moist, and in the meantime he had some major problems with corneal abrasions (causing painful light sensitivity) from the eyelid dragging over that dry little eye. Now he gets eyedrops every 2 to 3 hours during the day and a gooey eye ointment every night before bed. Missed drops mean eye damage, so he can’t do sleepovers or extended play times with any kid whose parents aren’t willing to give him his “drops and goop.” How this system is going to work when he’s too big to be in my care or the care of the school nurse all the time, I don’t know, but I’m not borrowing worries for now. One alternative the doctors have suggested we could seek in the next couple of years may be surgery to “plug” the ducts which drain the eye, so that what little moisture the eye has won’t just drain away so quickly.
Radiation-induced cataracts are progressive. Exposing these cataracts to extra sunlight may speed the progression. Sunlight can also aggravate glare symptoms from cataracts. Wearing sunglasses with UV protection when outside may help children and teens with cataracts.
I’ve had lots of radiation (left flank for neuroblastoma and cranial for leukemia) and years of chemotherapy. I have very bad vision as a result and have worn glasses since the age of 3. I also have small cataracts in both eyes, but they have never caused any problems. My eyes are also incredibly sensitive to sunlight.
Table of Contents
All Guides- 1. Survivorship
- 2. Emotions
- 3. Relationships
- 4. Navigating the System
- 5. Staying Healthy
- 6. Diseases
- 7. Fatigue
- 8. Brain and Nerves
- 9. Hormone-Producing Glands
- 10. Eyes and Ears
- 11. Head and Neck
- 12. Heart and Blood Vessels
- 13. Lungs
- 14. Kidneys, Bladder, and Genitals
- 15. Liver, Stomach, and Intestines
- 16. Immune System
- 17. Muscles and Bones
- 18. Skin, Breasts, and Hair
- 19. Second Cancers
- 20. Homage
- Appendix A. Survivor Sketches
- Appendix B. Resources
- Appendix C. References
- Appendix D. About the Authors
- Appendix E. Childhood Cancer Guides (TM)