Childhood Cancer Survivors
Skin And Glands
Skin is composed of two main layers: the epidermis and the dermis. The epidermis is a thin outer layer that is only 10 to 30 cells thick. The top layer of the epidermis is made up of dead cells full of keratin, a protein that keeps bacteria from entering the skin.
The thick, inner layer of the skin is called the dermis. Cells in the dermis produce melanin, a pigment that gives skin its color. Exposure to the sun increases the amount of melanin, causing a darkening of the skin. The dermis also contains nerve endings, blood vessels, and hair follicles. Sebaceous glands are usually attached to hair follicles in the dermis. These glands secrete oil that helps keep skin and hair from drying out.
Sweat glands produce a fluid containing water, salt, and waste products when the body is hot. When sweat evaporates, it cools the body. Blood vessels in the skin store blood to help regulate body temperature. During exercise, your skin appears flushed because the body pushes warm blood to the surface to cool off.
Damage to skin and nails
Skin can become discolored from some types of chemotherapy, higher doses of radiation, and graft-versus-host disease (GVHD), which occurs after some types of hematopoietic stem cell transplants.
Some children and adolescents treated with bleomycin or etoposide develop darkened areas of the skin (called hyperpigmentation). Pressure from trauma (such as removing a bandage from the skin) can result in darkened streaks in the traumatized areas. Bleomycin and etoposide can also cause darkening of the nail cuticles and creases on the palms. Dark bands on the nails may form as well. Doxorubicin (Adriamycin®), daunorubicin, and idarubicin can also cause darkening in skin creases, nails, palms, soles of feet, and face. These changes usually disappear over time.
Moles
Children or teens who had radiation therapy sometimes develop large numbers of brown moles on their bodies, often in unusual places such as the scalp, hands, or toes. It is important to know the difference between a normal mole and a skin cancer, but your provider should evaluate any concerning skin lesion. Know the signs you should be looking for. (See Figure 19-1 and Table 19-1) Many survivors, like the general public, develop dysplastic nevi which is a mole that does not look like a normal mole, has uneven edges and a combination of colors, ranging from pink to dark brown; may be larger than a normal mole, and is typically flat with a surface ranging from smooth to pebbly. Having at least 10 or more dysplastic nevi may increase your risk for developing skin cancer.
Table 19-1. ABCs of melanoma |
||
|---|---|---|
|
Melanoma characteristics |
Moles, noncancerous |
A = asymmetry |
Asymmetry – most melanomas are asymmetrical, if you draw a line down the center of the mole, each half looks very different from the other half. |
Most are round and symmetrical. Look similar on both halves. |
B = border |
Melanoma borders are uneven and may have scalloped or notched edges. |
Moles tend to have smoother, more even borders. |
C = color |
Multiple colors are a warning sign: different shades of brown, tan, or black colors. As it grows red, white or blue may appear |
Benign moles usually one shade of brown. |
D = diameter & dark |
A warning sign if the lesion is ¼ inch (6 millimeters; about the size of a pencil eraser) or more in diameter or larger should be evaluated. Also regardless of size, a lesion that is darker than others. |
|
E = evolving |
It is a warning if any spot on your skin changes size, shape, color or elevation (flat to raised) or if symptoms change such as itching, crusting, or bleeding. See your doctor right away. |
|
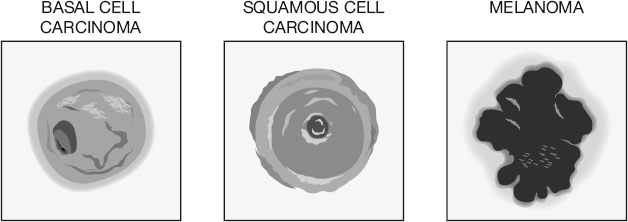
FIGURE 19-1. Three types of skin cancer: A. basal cell carcinoma, B. squamous cell carcinoma, and C. melanoma. (©Alex’s Lemonade Stand Foundation, 2025)
A. Basal cell carcinoma: Appearance: pearly, waxy bump with dark spot/red spot or flat brown lesion; Severity: least likely to spread; easy to treat.
B. Squamous cell carcinoma: Appearance: firm red pimple/nodule or scaly patch with darker crusted spot in center; Severity: easily treated if detected early; more likely to spread than basal cell carcinoma.
C. Melanoma. Appearance: black with very irregular borders with a lighter brown/red tone outline on the border, or a large brownish patch or smaller spot with black, red or white speckles. Other characteristics: an existing mole that bleeds, itches or changes shape/color. Severity: melanoma is the most serious form of skin cancer, needs diagnosis early, and can be difficult to treat and spreads easily/quickly.
Scarring and stretch marks
Most survivors have scars on their skin that serve as a daily reminder of their bout with cancer. Children or teens who had solid tumors may have extensive scarring from the tumor removal surgery. Those who had leukemia or lymphomas have scars from central line insertion and removal. Some children and teens who get severe cases of shingles have scarring along the nerve tracts. Mild and moderate cases usually heal without scarring.
Many survivors who had radiotherapy (except those who had cranial radiation only or total body irradiation) have permanent tattoos (small black dots) on their skin to outline the treatment areas. Some children and teens gain weight when they are on steroids (i.e., prednisone, dexamethasone) for extended periods of time. This can cause stretch marks. This is a variable side effect—some children gain weight but have no stretch marks, while others get them all over the body. Stretch marks sometimes fade with time.
I always hated the way I looked and the scars I have. I came to realize that they meant I won a hard battle, but I didn’t truly love them until I met my husband. He pointed out all the things he loved about me and my scars were one of them.
Radiation injuries to the skin
Survivors of childhood cancer who had high-dose radiation frequently have acute skin problems (e.g., redness, peeling) during treatment. Chronic radiation injury to the skin and underlying tissues can occur months or years after the radiation is given.
Signs and symptoms of radiation injury to the skin:
Dry skin
Dark and/or light areas on the skin
Thinning of the skin
A spidery pattern of capillaries visible in the skin (telangiectasia)
Ulcers on the skin
The first late effect to the skin after radiation is usually a loss of elasticity. Areas of the skin can become tough (called fibrosis) and the tissues can contract. In some cases, telangiectasia appears, small red or purple clusters, often spidery in appearance on the skin.
Radiation can also cause the skin to age faster. Skin in the areas radiated may become drier and more wrinkled and may develop age spots. These late effects are much more likely in survivors who had high-dose radiation. Late effects to the skin depend on dose per fraction (the amount of radiation given at one time) and the total dose. Current technology uses megavoltage (skin-sparing) radiation to avoid severe damage to the skin.
Tissue damage under the skin can make the skin tighter and more vulnerable to breakdown. Factors that contribute to ulcers in the radiation field are trauma, pressure, ultraviolet light (from sunlight or tanning beds), and exposure to intense cold.
Damage to sweat glands, sebaceous glands and hair follicles
Radiation can also damage or destroy sweat glands, sebaceous glands, and hair follicles. Damage to these glands may be permanent. Itchy skin can persist for years after treatment with radiation. It is most common in those who had high-dose radiation or GVHD after an allogeneic bone marrow transplant.
Risk of skin cancer
A serious late effect to the skin after treatment for childhood cancer is skin cancer (although it can develop in people who never had childhood cancer). Radiation increases the risk and shortens the development time of skin cancers. Skin cancers can arise in irradiated or non-irradiated skin, and exposure to the sun may hasten their development. Having a family history of skin cancers and getting older also increase your risk of developing skin cancers. See Chapter 20, Subsequent Malignancies, for more information about skin cancers.
Medical management of damage to skin and glands
Careful evaluation of skin changes should be part of your yearly follow-up examination. In some cases, referral is made to a dermatologist for more frequent examinations. Any changes in color, scarring, dryness, fibrosis, or tightness should be identified and recorded in your medical chart. Reversal of late effects to the skin is not possible, but education about ways to slow the process can help.
Protect your skin from the sun. If you had radiation, you have a definite risk of cancers of the skin, especially in the irradiated areas. Try to limit your sun exposure, and use sunscreen of at least SPF (sun protection factor) 30 when you are out in the sun. If you had radiation to the chest or back, always wear a shirt when in the sun. If you had radiation to the arms or legs, keep them covered. Anyone who had cranial radiation or who has thin hair should wear a hat when outdoors.
Scars need extra protection from the sun. Normal skin sloughs off if sunburned, but scars cannot do that. They may remain darker. If you are going out in the sun for extended periods with your scars exposed, it’s best to put zinc oxide on them.
Inspect moles regularly. If you have lots of moles on your skin, be sure to inspect them regularly. The moles probably won’t become cancerous, but it is best to keep an eye on them. Always point them out to your healthcare provider at your follow-up visits, especially ones not normally noticed—for example, between your toes or on your scalp. Ask your healthcare provider to check areas you can’t see such as on your back or back of the neck. If moles change shape, color, or size, make an appointment with a dermatologist. Some dermatologists take photographs of a survivor’s moles so they can do a yearly comparison. Moles need continued surveillance, and you should always use sunscreen to protect your skin and moles from ultraviolet rays.
Dry skin and treatment for scars and/or stretch marks. If sebaceous gland damage makes your skin especially dry, using a moisturizing cream may make you more comfortable. Dermatologists sometimes treat scars, stretch marks, and other skin problems with medicated creams. If your scars and/or stretch marks bother you, check with your dermatologist to see if there are any medications available that might help to fade them. You could also consult a plastic surgeon to learn about any surgical options for removal of scars and/or stretch marks.
Precautions before surgery. Make sure to tell your surgeon about your cancer history if she needs to operate on previously irradiated skin. Special precautions must be taken as the tissue might be fragile and slow to heal.
Table of Contents
All Guides- Acknowledgements
- Contributors
- Foreword
- Preface
- 1. Survivorship
- 2. Emotions
- 3. Relationships
- 4. Navigating The System
- 5. Staying Healthy
- 6. Genetic Testing And Childhood Cancer
- 7. Diseases
- 8. Fatigue
- 9. Brain And Nerves
- 10. Hormone-Producing Glands
- 11. Eyes And Ears
- 12. Head And Neck
- 13. Heart And Blood Vessels
- 14. Lungs
- 15. Kidneys, Bladder, And Genitals
- 16. Liver, Stomach, And Intestines
- 17. Immune System
- 18. Muscles And Bones
- 19. Skin, Breasts, And Hair
- 20. Subsequent Malignancies
- About The Editors